
Case Report | DOI: https://doi.org/10.31579/2693-7247/012
1 University hospital establishment Oran pharmacovigilance service Pharmaceutical development research laboratory, Oran University 1 Algeria.
*Corresponding Author: Toumi. H., University hospital establishment Oran pharmacovigilance service Pharmaceutical development research laboratory, Oran University 1 Algeria.
Citation: Bekhtaoui. C., Bouguedra. H., Chadou. H., Boudia F., Derbale.F and Toumi.H, (2020) Hydroxychloroquine and chronic renal failure, J, Pharmaceutics and Pharmacology Research 3(1); DOI: 10.31579/2693-7247/012
Copyright: © 2020, Toumi. H. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 August 2020 | Accepted: 24 August 2020 | Published: 08 September 2020
Keywords: Keyword
In Algeria, the essentially hydroxychloroquine therapeutic protocol was adopted since March 23, 2020, to which patients with Covid-19 were subjected.
In Algeria, the essentially hydroxychloroquine therapeutic protocol was adopted since March 23, 2020, to which patients with Covid-19 were subjected. This protocol has proven its "almost total" effectiveness by noting a recovery of 98.2% out of a total of 16,000 cases treated [1].
Hydroxychloroquine (HCQ) is preferred for its better expected tolerance, based on the publications of preliminary work by several teams that we analyzed previously with a further three months' follow-up.
On the pharmaceutical level, the pharmacology of this molecule is of interest and emphasizes the interest of pharmacokinetic studies to define the optimal dosage regimen for patients with a particular statue (Renal Insufficiency - Hepatic Insufficiency - Fatty) COVID-19. On the basis of this work, dosage adjustments can be proposed and the chronology of administration can be optimized with therapeutic monitoring of the drugs to be performed to personalize the individual dosage regimen.
Therefore, the role of the hospital pharmacist is essential in the pandemic context to optimize and modify practices by developing new prescribing protocols while ensuring that adverse events are well managed.
This is an 18 year old patient with a weight of 65kg confirmed COVID-19 positive suffering from a malformative nephropathy, admitted on 05/11/2020 to the service COVID university hospital Establishment UHE, ORAN, Algeria after suspicion contamination whose father is confirmed positive.
The patient being asymptomatic with a general preserved state, diuresis 1100 ml, an arterial pressure = 120/80, a temperature: 36.2 ° c, a heart rate = 90 bpm, an oxygen saturation SAO2 = 98%, and presenting at l '' ECG a regular sinus rhythm (PR = 0.16 s, QRSfin, normal AXIS, QTc = 400ms).
The patient was put on specific treatment according to the national protocol. The latter will use the following drugs: Hydroxychloroquine 200mg at a rate of 200 mg x 3 times per day for 10 days in combination with Azithromycin 250 mg: 500 mg on the first day followed by 250 mg per day for the next 4 days,
In view of the severe renal impairment (clearance=8ml/min) it was recommended a dosage adjustment of HCQ following nephrological advice, i.e. a 50% reduction of the standard dose to 100mg HCQ three times daily.
After a request from the Therapeutic Optimisation Unit of the UHE Pharmacovigilance Department, capsules with the recommended dosage were prepared; combined with a pharmaceutical analysis of the patient's medical prescription by the clinical pharmacy team.
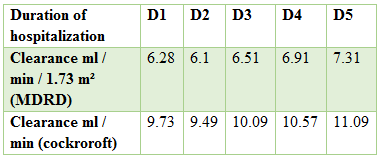
The evolution of the patient's clearance during the first five days of hospitalisation was as follow
Hydroxychloroquine is an anti-malarial from the class of amino-4-quinolines which has found its place in the ministerial protocol proposed by the expert committee in response to the COVID-19 pandemic [2].
This molecule is rapidly absorbed in the digestive tract after oral administration, it has a large volume of distribution and it is strongly linked to plasma proteins with a strong distribution in the following tissues: kidney, liver, lungs, cells containing melanin such as those of the eyes and the skin. It crosses the placenta. It is mainly metabolized in monodesethylchloroquine (cletoquine) and bisdesethylchloroquine in the liver. Monodesethylcholoroquine has been reported to have some activity.
Elimination is mainly renal: 50% in unchanged form and 10% in monodesethylchloroquine form. The half-life of hydroxychloroquine is approximately 30 days. This molecule therefore accumulates in the tissues and can be found several weeks to months in the tissues. Hydroxychloroquine is a substrate for CYP2C8, CYP3A4 and CYP2C6, possible pharmacokinetic drug interactions should be taken into account [2, 3].
The serious side effects that hydroxychloroquine can cause, mainly cardiac arrhythmias, are known, in particular the risk of prolonging the QTc interval. And these effects can be further enhanced by the simultaneous administration of other drugs such as azithromycin. In addition, these two active ingredients can damage the liver, kidneys or nervous system and cause a drop in blood sugar. Serious signs of cardiac toxicity have been reported in blood concentrations of hydroxychloroquine ranging from 2.05 to 29.40 mcmol / l. It is recommended to monitor plasma concentrations in patients receiving this treatment for COVID-19 and to provide cardiac monitoring [3, 4].
Whipple's disease, a systemic infectious disease caused by Tropheryma whipplei or the standard treatment, is the combination of doxycycline and hydroxychloroquine. In this indication, the HCQ is administered at the same dosage as in the proposed covid_19 protocol (600 mg per day). The target HCQ plasma levels described in the literature are 1 +/- 0.2 ug / ml [5].
HCQ is mainly excreted via the kidneys. Particular attention paid to patients with renal insufficiency conducive to developing early cardiotoxicity. It was recommended to use lower doses of HCQ [6,7] varying according to the glomerular filtration rate (table 1) and the type of dialysis (table 2) it is described in the literature that dialysis does not significantly lower plasma concentrations. The dose reductions illustrated in the tables are recommended in the context of systemic inflammatory pathologies such as lupus, an indication in which the taking of HCQ is long-term with low dosages (200 mg) and in single dose for objective of avoid cumulative retinal toxicity.Due to the lack of experience with dosage adjustment and in order to avoid early cardiac toxicity in patients with renal failure; a 50% reduction in HCQ has been proposed. Cardiac evaluation of this patient showed no abnormalities.


Therapeutic optimization of hydroxychloroquine
At the pharmacovigilance service for the therapeutic optimization unit, a preparation of hydroxychloroquine dosed at 100 mg was carried out according to the following steps:
I-Calculation of the total mass of the active principle
Total mass of the active ingredient = unit dosage requested * number of capsules to be prepared
= 100 * 30 = 3000mg
Knowing that:
The number of capsules to prepare = dosage * duration of treatment
= 3 * 10 = 30
II-Deconditioning of a specialty
It is the calculation of the number of tablets to be crushed or capsules to empty of their content:
N Cp = unit dosage requested * number of capsules to prepare
Initial drug dosage
N Cp = 100 * 30/200 = 15cp
III-Adjustment of the volume of the diluent to be added
Depending on the size of the desired capsule, the volume of the diluent to be added can be calculated.
For a capsule N ° 1 we need 0.5ml of diluent for each capsule.
For 30 capsules you need 15ml of diluent.
IV-Trituration with mortar of the active ingredient + diluent
V-Preparation of the capsule filler
VI-Filling and ejection of capsules
VII-Pillbox
VIII-Labeling
Medical prescription:
Our team carried out the pharmaceutical analysis, various problems related to the drug were detected:
Combination type not recommended (hydroxychloroquine / azithromycin).Hydroxychloroquine can prolong the QT interval. Theoretically, co-administration with other drugs that may prolong the QT interval (azithromycin) may result in additive effects and an increased risk of ventricular arrhythmias, including torsade de pointes and sudden death. In general, the risk of an individual drug or combination of drugs causing a ventricular arrhythmia associated with QT prolongation is largely unpredictable, but may be increased by certain underlying risk factors, such as congenital long QT syndrome, heart disease and electrolyte disturbances (e.g., hypokalemia, hypomagnesemia). In addition, the extent of drug-induced QT prolongation depends on the drug involved and its dosage.Pharmaceutical intervention:
The calculated score of the patient in question being equal to 6 is equivalent to a low score: Low risk of prolongation of the QT interval; always consider that a higher risk may develop based on clinical course and drug interactions and pharmacokinetics.
On this basis we recommend:
- The ECG, repeated 8 to 12 hours after the start of QT prolongation therapy to look for signs of QT prolongation, with closer monitoring if observed.
- Correct electrolyte abnormalities and maintain blood potassium> 4.0 mEq / L and serum magnesium> 2.0 mg / d.
Lovenox 4000 IU / d / d for 10 days [12].Reminder:
The risk factors of patients who are candidates for prophylaxis are well known [13, 14 and 15]: age, acute infection, active cancer, history of venous thromboembolic disease (VTE), prolonged immobilization, chronic heart failure and insufficiency respiratory.
The patient in question has two risk factors (covid-19 infection and hospitalization); which calls for the need for thromboprophylaxis:
-Description of the problem with the drug treatment: the patient being insufficient renal end, it is not recommended to use heparin at low molecular weight because of the increase in the risk of haemorrhage.
The patient's clearance being less than 15 ml / min (8ml / min): a substitution with HNF SC (Calciparin according to the establishment's register) is recommended, the recommended dosage is shown in the table below for the thromboembolic risk:

High risk: in case of: active cancer, history of VTE, recent surgery, known thrombophilia.
That said, our patient with a low thromboembolic risk, we recommend a dosage of 5000U 2 * / d.
Kalemia, Platelet count before treatment and 2 * / week during treatment, Liver balance before treatment, monitoring of anti-Xa or TCA is not recommended when heparin is used for preventive purposes [16].
Cefotaxime (Claforan) 1G 3 * d for 10 days [17].
In patients with a clearance of less than 10 ml / min; after a normal starting dose, maintenance doses should be reduced by half compared to the normal dose without changing the dose interval. A dosage of 500 mg / 3 * d is recommended after an initial dose of 1G / 3 * d.
- Liver balance: hydroxychloroquine is metabolized in the liver, it is necessary to evaluate the liver balance before starting treatment. Liver failure causes an accumulation of hydroxychloroquine in the tissues, which is equivalent to an overdose [2].
- Magnesemia: it is necessary to perform magnesemia coupled with a kalemia for optimal cardiac monitoring [8].
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
